Internal Documents Further Contradict Fauci’s ‘Gain-of-Function’ Research Denials
Caroline Downey
·3 min read
In this article:
Newly
released documents appear to contradict Dr. Anthony Fauci’s repeated
claims that the NIH did not fund gain-of-function research on bat
coronaviruses at the Wuhan Institute of Virology (WIV).
The
internal documents detail the work of EcoHealth Alliance, an American
research non-profit which used NIH funding to research novel bat
coronaviruses at the Wuhan lab. Among the documents, which were obtained
by The Interceptthrough
a Freedom of Information Act request, is a previously unpublished
EcoHealth Alliance grant proposal filed with the National Institute of
Allergy and Infectious Disease, which is run by Fauci.
The
proposal requests $3.1 million for a project titled “Understanding the
Risk of Bat Coronavirus Emergence,” which involved screening thousands
of lab workers for novel bat coronaviruses. The grant was awarded for
five years, from 2014 to 2019, and was subsequently renewed before being
suspended by the Trump administration. The proposal directs $599,000 of
the total grant to the Wuhan Institute of Virology for research
designed to make the viruses more dangerous and/or infectious — and its
author acknowledged the danger associated with such work.
“Fieldwork
involves the highest risk of exposure to SARS or other CoVs, while
working in caves with high bat density overhead and the potential for
fecal dust to be inhaled,” it read.
After reviewing the documents,
Gary Ruskin, executive director of a group probing COVID’s origins
called U.S. Right to Know, told the Intercept that the grant was a “road map to the high-risk research that could have led to the current pandemic.”
Fauci
has repeatedly insisted during his Senate testimony that the research
being funded by the NIH at the WIV did not qualify as “gain-of-function”
under the NIH’s current definition. But critics, including Senator Rand
Paul of Kentucky, have accused Fauci of playing semantic games by
excluding research which makes bat coronaviruses more transmissible —
the commonly accepted definition of “gain-of-function” — from his more
convenient definition.
Dr. Richard Ebright, biosafety expert and
professor of chemistry and chemical biology at Rutgers University, has
also disputed Fauci’s claims. Primarily, he has rebutted Fauci’s chief
declaration that the NIH “has not ever and does not now fund gain of
function research in the Wuhan Institute of Virology [WIV]” as
“demonstrably false.”
Ebright told National Review that
the NIH-financed work at the WIV “epitomizes” the definition of
gain-of-function research, which involves working with “enhanced
potential pandemic pathogen (PPP)” or those pathogens “resulting from
the enhancement of the transmissibility and/or virulence of a pathogen.”
The
Wuhan lab’s program qualified as gain-of-function research because it
artificially engineered novel SARS-related coronaviruses to make them
more transmissible and dangerous to humans, the breeding ground for
accident, Ebright said.
Following the FOIA release secured by the Intercept,
Ebright doubled down on his repudiation of Fauci, confirming that the
NIH did conduct gain-of-function research during the five-year period in
question.
“The materials show that the 2014 and 2019 NIH grants
to EcoHealth with subcontracts to WIV funded gain-of-function research
as defined in federal policies in effect in 2014-2017 and potential
pandemic pathogen enhancement as defined in federal policies in effect
in 2017-present,” Ebright tweeted.
He added
that the “documents make it clear that assertions by the NIH Director,
Francis Collins, and the NIAID Director, Anthony Fauci, that the NIH did
not support gain-of-function research or potential pandemic pathogen
enhancement at WIV are untruthful.”
As evidence mounts in favor of
Ebright’s conclusion, further discrediting Fauci, some Republican
lawmakers have called for the doctor’s removal from his post in the
Biden administration. Shortly after the FOIA disclosure, GOP Senator
Josh Hawley demanded that Fauci step down and be subject to a
congressional investigation for lying to the public about the NIH’s
activities.
“Anthony Fauci has repeatedly and deliberately mislead
Congress and the American people. Resign. And face a congressional
inquiry,” he tweeted.
'Tucker
Carlson Tonight' guest host Brian Kilmeade reacts to a report
indicating the NIH funded COVID research at the Wuhan Institute of
Virology
"Tucker Carlson Tonight" host Brian Kilmeade blasted National Institute of Allergy and Infectious Diseases chief Dr. Anthony Fauci after a new report from The Intercept revealed U.S. tax dollars were used to back bat coronavirus research at the Wuhan Institute of Virology.
KILMEADE:
After reviewing the internal N.I.H. documents published today by The
Intercept, one molecular biologist, Alina Chan, made this assessment:
"In
this proposal, they actually point out that they know how risky this
work is. They keep talking about people potentially getting bitten — and
they kept records of everyone who got bitten," Chan said. "Does
EcoHealth have those records? And if not, how can they possibly rule out
a research-related accident?"
Some of this is dangerous
research, according to Richard Ebright, and was occurring in facilities
that have the same safety precautions as the average dentist's office.
…
It
now appears that Tony Fauci was lying under oath. According to Richard
Ebright, "the documents make it clear that assertions by the NIH
Director, Francis Collins, and the NIAID Director, Anthony Fauci, that
the NIH did not support gain-of-function research or potential pandemic
pathogen enhancement at [the Wuhan Institute of Virology] are
untruthful."
Do we want
public health officials to report facts and uncertainties transparently?
Or do we want them to shape information to influence the public to take
specific actions?
In March 2020, as the pandemic began, Anthony Fauci, the chief medical adviser to the president of the United States, explained in a 60 Minutes interview that he felt community use of masks was unnecessary. A few months later, he argued
that his statements were not meant to imply that he felt the data to
justify the use of cloth masks was insufficient. Rather, he said, had he
endorsed mask wearing (of any kind), mass panic would ensue and lead to
a surgical and N95 mask shortage among health care workers, who needed
the masks more. Yet, emails from a Freedom of Information Act request
revealed that Fauci privately gave the same advice—against mask
use—suggesting it was not merely his outward stance to the broader
public.
Although
some have claimed that the evidence changed substantively in the early
weeks of March, our assessment of the literature does not concur. We
believe the evidence at the time of Fauci’s 60 Minutes interview
was largely similar to that in April 2020. Thus, there are two ways to
consider Fauci’s statement. One possibility is, as he says, that his
initial statement was dishonest but motivated to avoid a run on masks
needed by health care workers. The other is that he believed his initial
statements were accurate, and he subsequently decided to advocate for
cloth masks to divert attention from surgical or N95 masks, or to
provide a sense of hope and control to a fearful and anxious public.
Advertisement
Additional
evidence suggests that the second interpretation may be more accurate.
In a lengthy commentary from July 2020, COVID expert Michael Osterholm wrote
in detail about the continued scientific uncertainty regarding
masks—even as he expressed support for their widespread public use as
one measure among many. But Fauci’s reversal, which came at a time of
political polarization, contributed to the evolution of masks from a
basic, precautionary mitigation strategy to a badge of political
allegiance. President Donald Trump was reluctant to wear a mask and
justified his behavior by referring to Fauci’s comments from the 60 Minutes interview. The controversy continued into the presidential debates, with Trump mocking Joe Biden for donning the “biggest mask” he’d ever seen.
One
thing is beyond a doubt, however: One of those two statements did not
accurately reflect the evidence as Fauci saw it. Such high-profile mixed
messages in a short time frame, without substantive new data to justify
the change, generated confusion and a backlash from politicians, other
experts, and the general public.
Do we want public health officials to report facts and uncertainties transparently? Or do we want them to shape information?
When
experts or agencies deliver information to the public that they
consider possibly or definitively false to further a larger, often
well-meaning agenda, they are telling what is called a noble lie.
Although the teller’s intentions may be pure—for example, a feeling of
urgency that behavioral change is needed among the lay public—the
consequences can undermine not only those intentions but also public
trust in experts and science. During the first year of COVID-19, leaders
were faced with an unknown disease amid a politically sensitive
election in the era of social media, and the preconditions for noble
lies became especially fertile. Not surprisingly, we witnessed several
examples. More than anything, these examples illustrate the destructive
potential of such lies.
When polls said only about half of all
Americans would take a vaccine, I was saying herd immunity would take 70
to 75 percent. Then, when newer surveys said 60 percent or more would
take it, I thought, “I can nudge this up a bit,” so I went to 80, 85.
In
his own words, he “nudged” his target range for herd immunity to
promote vaccine uptake. Even though his comments were made to influence
public actions to get more people vaccinated (a noble effort), the
central dilemma remains: Do we want public health officials to report
facts and uncertainties transparently? Or do we want them to shape
information, via nudges, to influence the public to take specific
actions? The former fosters an open and honest dialogue with the public
to facilitate democratic policymaking. The second subverts the very idea
of a democracy and implies that those who set the rules or shape the
media narrative are justified in depriving the public of information
that they may consider or value differently.
Aside
from whether it’s right to tell noble lies in the service of eliciting
socially beneficial behavior, there is also the question of efficacy.
Experts on infectious diseases are not necessarily experts on social
behavior. Even if we accept Fauci’s claim that he downplayed the
importance of wearing masks because he didn’t want to unleash a run on
masks, we might wonder how he knew that his noble lie would be more
effective than simply being honest and explaining to people why it was
important to assure an adequate supply of masks for medical workers.
With
the arrival of vaccines in early 2021, the potential for such
deliberately misleading messages to backfire became more obvious. Key
opinion leaders, agencies, and the Centers for Disease Control and
Prevention all articulated some version of “once you are vaccinated,
nothing changes,” implying that experts did not know if it was safe to
relax precautions and restrictions, such as mask wearing or social
distancing, after immunization. But the stance was immediately called into question by others, including epidemiologists,
who pointed to the high efficacy of the vaccines and suggested that
some, but not all, social distancing measures could be relaxed in
certain circumstances. Ultimately, the “no change” message, which may
have been intended to discourage mass gatherings or out of a fear that
unvaccinated people would lie about their vaccination status, may itself
have been harmful: Surveys find that interest in vaccination increases if people are told that it means they can stop masking.
Advertisement
The fourth noble lie from government agencies and/or officials occurred
more recently. On June 4, using data from February to March, the agency
made the case that hospitalizations were rising in adolescents. It
tweeted, “The report shows the importance of #COVID19 vaccination for
adolescents.” That tweet spurred a great deal of media attention and
concern. It was true that hospitalization rates had risen. However, at the time of the press coverage, hospitalization rates in this age group had already fallen again. Numerous commenters
immediately pointed out that the “rise” in hospitalization statistic
promoted by the CDC was out of date the moment it was highlighted and
raised questions about why the CDC would promote a dated statistic, when
the organization had access to up-to-date information.
This obvious error was compounded weeks later during a meeting of the Advisory Committee on Immunization Practices.
The committee met to discuss what we knew and did not know about heart
inflammation, or myocarditis, that had been linked to mRNA vaccination,
and most notable in young men who received the vaccine. During the
course of the meeting, representatives of the CDC showed a model that
claimed that vaccination of young adults was preferable to the disease
itself.
There
were, however, several concerns with this model. First, it used rates
of community SARS-CoV-2 spread that again were out of date. By the time
of the meeting, the rates were lower, meaning the benefits of
vaccination would be reduced, but the harms remain the same. Second, it
did not consider the risks separately for boys and girls, who appear to
have substantially different risk of myocarditis (much higher in boys).
Third, it did not consider any middle ground positions, such as only
receiving one dose of the vaccine, which provides much of the benefit
with far lower myocarditis risk. Instead, the CDC presented zero or two
doses as the only options. Fourth, the modeling did not consider natural
immunity—i.e., the vaccine’s risk to kids who already recovered from
COVID-19 might be the same, but the benefits far lower (as these
children have some natural immunity). Finally, the model did not
consider the fact that young adults with preexisting medical conditions
and those who are otherwise well might have different risk benefit
profiles, as the former account for a disproportionate number of
COVID-19 hospitalizations.
Advertisement
Together,
these are all information choices made by government agencies and/or
officials about vaccination of young adults. Amplifying out-of-date
statistics and building a model to support vaccination that has
questionable assumptions work to support rapid deployment of two doses
of mRNA to all healthy kids aged 12 to 17. That may be the CDC’s policy
pursuit, and one we are sympathetic to. However, distorting evidence to
achieve this result is a form of a noble lie. Accurately reporting
current risks to adolescents, and exploring other dosing possibilities,
is part of the unbiased scientific exploration of data.
We
worry that vaccine policy among supporters of vaccines is increasingly
anchored to the irrational views of those who oppose them—by always
pursuing the opposite. Exaggerating the risk of the virus in the moment
and failing to explore middle ground positions appear to be the
antithesis of the anti-vax movement, which is an extremist effort to refuse vaccination.
This seems a reflexive attempt to vaccinate at all costs—by creating
fear in the public (despite falling adolescent rates) and pushing the
notion that two doses of mRNA at the current dose level or nothing at
all are the only two choices—a logical error called the fallacy of the
excluded middle.
Noble
lies—small untruths—yield unpredictable outcomes. Nietzsche once wrote,
“Not that you lied to me, but that I no longer believe you, has shaken
me.”Public health messaging is predicated on trust, which
overcomes the enormous complexity of the scientific literature, creating
an opportunity to communicate initiatives effectively. Still, violation
of this trust renders the communication unreliable. When trust is
shattered, messaging is no longer clear and straightforward, and instead
results in the audience trying to reverse-engineer the statement based
on their view of the speaker’s intent. Simply put, noble lies can rob
confidence from the public, leading to confusion, a loss of credibility,
conspiracy theories, and obfuscated policy.
Noble
lies are a trap. We cannot predict the public’s behavior, and loss of
trust is devastating. The general population is far too skeptical to
blindly follow the advice of experts, and far too intelligent to be
easily duped.
Children
in Copenhagen play during the SARS-CoV-2 pandemic. Endemic viruses are
often first encountered in childhood. Credit: Liselotte Sabroe/Ritzau
Scanpix/AFP/Getty
For much of the past year, life in Western
Australia has been coronavirus-free. Friends gathered in pubs; people
kissed and hugged their relatives; children went to school without
temperature checks or wearing masks. The state maintained this enviable
position only by placing heavy restrictions on travel and imposing
lockdowns — some regions entered a snap lockdown at the beginning of the
year after a security guard at a hotel where visitors were quarantined
tested positive for the virus. But the experience in Western Australia
has provided a glimpse into a life free from the SARS-CoV-2 coronavirus.
If other regions, aided by vaccines, aimed for a similar zero-COVID
strategy, then could the world hope to rid itself of the virus?
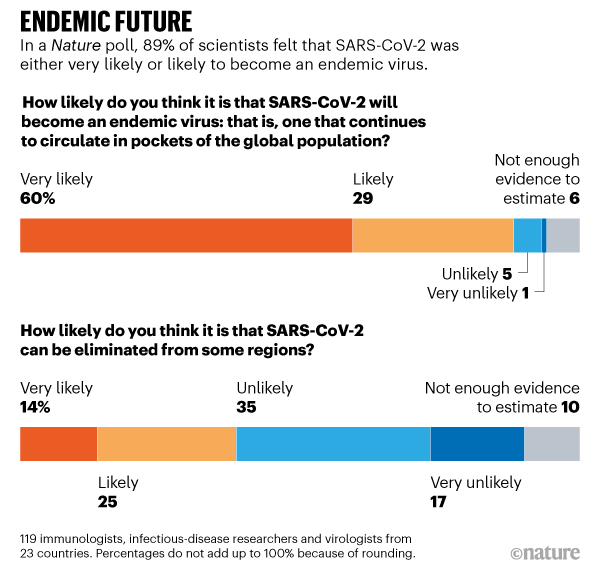
It’s a beautiful dream but most scientists think it’s improbable. In January, Nature
asked more than 100 immunologists, infectious-disease researchers and
virologists working on the coronavirus whether it could be eradicated.
Almost 90% of respondents think that the coronavirus will become endemic
— meaning that it will continue to circulate in pockets of the global
population for years to come (see 'Endemic future').
Source: Nature survey
“Eradicating this virus right now from the world is a lot
like trying to plan the construction of a stepping-stone pathway to the
Moon. It’s unrealistic,” says Michael Osterholm, an epidemiologist at
the University of Minnesota in Minneapolis.
But failure to
eradicate the virus does not mean that death, illness or social
isolation will continue on the scales seen so far. The future will
depend heavily on the type of immunity people acquire through infection
or vaccination and how the virus evolves. Influenza and the four human
coronaviruses that cause common colds are also endemic: but a
combination of annual vaccines and acquired immunity means that
societies tolerate the seasonal deaths and illnesses they bring without
requiring lockdowns, masks and social distancing.
More than one-third of the respondents to Nature’s
survey thought that it would be possible to eliminate SARS-CoV-2 from
some regions while it continued to circulate in others. In zero-COVID
regions there would be a continual risk of disease outbreaks, but they
could be quenched quickly by herd immunity if most people had been
vaccinated. “I guess COVID will be eliminated from some countries, but
with a continuing (and maybe seasonal) risk of reintroduction from
places where vaccine coverage and public-health measures have not been
good enough,” says Christopher Dye, an epidemiologist at the University
of Oxford, UK.
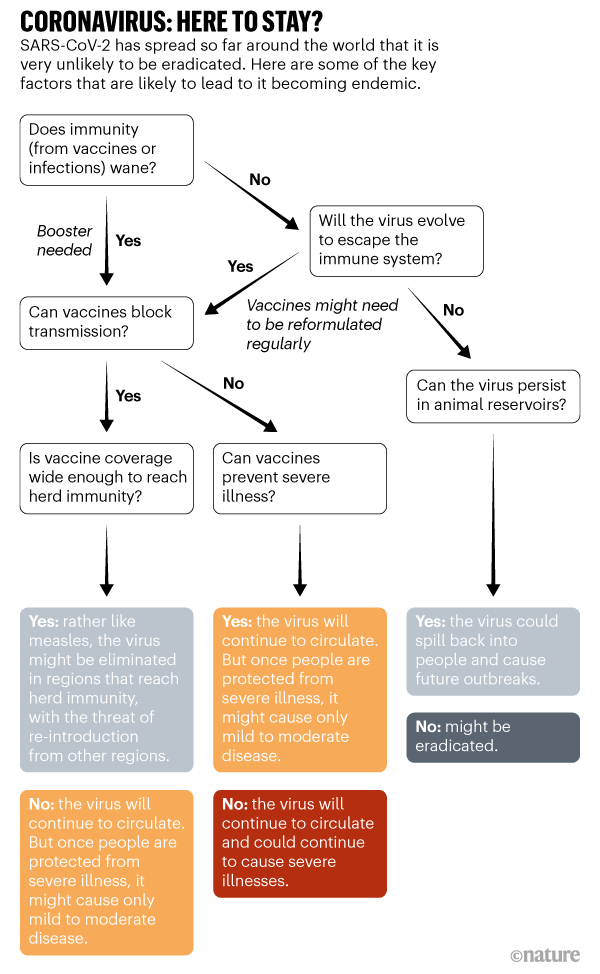
“The virus becoming endemic is likely, but the
pattern that it will take is hard to predict,” says Angela Rasmussen, a
virologist from Georgetown University, who is based in Seattle,
Washington. This will determine the societal costs of SARS-CoV-2 for 5,
10 or even 50 years in the future (see ‘Coronavirus: here to stay?’).
Childhood virus
Five years from now, when
childcare centres call parents to tell them that their child has a runny
nose and a fever, the COVID-19 pandemic might seem a distant memory.
But there’s a chance the virus that killed more than 1.5 million people
in 2020 alone will be the culprit.
This is one scenario that
scientists foresee for SARS-CoV-2. The virus sticks around, but once
people develop some immunity to it — either through natural infection or
vaccination — they won’t come down with severe symptoms. The virus
would become a foe first encountered in early childhood, when it
typically causes mild infection or none at all, says Jennie Lavine, an
infectious-disease researcher at Emory University in Atlanta, Georgia.
Scientists
consider this possible because that’s how the four endemic
coronaviruses, called OC43, 229E, NL63 and HKU1, behave. At least three
of these viruses have probably been circulating in human populations for
hundreds of years; two of them are responsible for roughly 15% of
respiratory infections. Using data from previous studies, Lavine and her
colleagues developed a model that shows how most children first come
down with these viruses before the age of 6 and develop immunity to them1.
That defence wanes pretty quickly so it is not sufficient to block
reinfection entirely, but it seems to protect adults from getting sick,
says Lavine. Even in children, the first infection is relatively mild.
Whether immunity to SARS-CoV-2 will behave in the same way is
so far unclear. A large study of people who have had COVID-19 suggests
that their levels of neutralizing antibodies — which help to block
reinfection — start to decline after around six to eight months2. But their bodies also make memory B cells, which can manufacture antibodies if a new infection arises, and T cells that can eliminate virus-infected cells,
says Daniela Weiskopf, an immunologist at the La Jolla Institute for
Immunology in California, who co-authored the study. It’s yet to be
established if this immune memory can block viral reinfection — although
cases of reinfection have been recorded, and new viral variants might
make them more likely, they are still considered rare.
Weiskopf
and her colleagues are still tracking the immune memory of people
infected with COVID-19 to see if it persists. If most people develop
life-long immunity to the virus, either through natural infection or
vaccination, then the virus is unlikely to become endemic, she says. But
immunity might wane after a year or two — and already there are hints that the virus can evolve to escape it. More than half the scientists who responded to Nature’s survey think waning immunity will be one of the main drivers of the virus becoming endemic.
Because
the virus has spread around the world, it might seem that it could
already be classed as endemic. But because infections continue to
increase worldwide, and with so many people still susceptible,
scientists still technically class it as in a pandemic phase. In the
endemic phase, the number of infections becomes relatively constant
across years, allowing for occasional flare-ups, says Lavine.
To
reach this steady state could take a few years or decades, depending on
how quickly populations develop immunity, says Lavine. Allowing the
virus to spread unchecked would be the fastest way to get to that point —
but that would result in many millions of deaths. “That path has some
huge costs,” she says. The most palatable path is through vaccination.
Vaccines and herd immunity
Countries
that have begun distributing COVID-19 vaccines soon expect to see a
reduction in severe illness. But it will take longer to see how
effectively vaccines can reduce transmission. Data from clinical trials
suggest that vaccines that prevent symptomatic infection might also stop
a person from passing on the virus.
If vaccines do block transmission — and if they remain
effective against newer variants of the virus — it might be possible to
eliminate the virus in regions where enough people are vaccinated so
that they can protect those who are not, contributing to herd immunity. A
vaccine that is 90% effective at blocking transmission will need to
reach at least 55% of the population to achieve temporary herd immunity
as long as some social distancing measures — such as face masks and many
people working from home — remain in place to keep transmission in
check, according to a model3
developed by Alexandra Hogan at Imperial College London and her
colleagues. (A vaccine would need to reach almost 67% of people to
provide herd immunity if all social distancing measures were lifted.)
But if the rate of transmission increases because of a new variant, or
if a vaccine is less effective than 90% at blocking transmission,
vaccine coverage will need to be greater to blunt circulation.
Vaccinating
even 55% of the population will be challenging in many countries. “The
virus will stick around if parts of the world don’t get vaccinated,”
says Jeffrey Shaman, an infectious-disease researcher at Columbia
University in New York City.
Even if the virus remains endemic in
many regions, global travel will probably resume when severe infections
are reduced to levels that health services can cope with, and when a
high proportion of people who are vulnerable to severe illness have been
vaccinated, says Dye.
Similar to flu?
The 1918
influenza pandemic, which killed more than 50 million people, is the
yardstick by which all other pandemics are measured. It was sparked by a
type of virus known as influenza A, which originated in birds. Almost
all cases of influenza A since then, and all subsequent flu pandemics,
have been caused by descendants of the 1918 virus. These descendants
circulate the globe, infecting millions of people each year. Flu
pandemics occur when populations are naive to a virus; by the time a
pandemic virus becomes seasonal, much of the population has some
immunity to it. Seasonal flu still has a significant toll globally,
claiming roughly 650,000 lives per year.
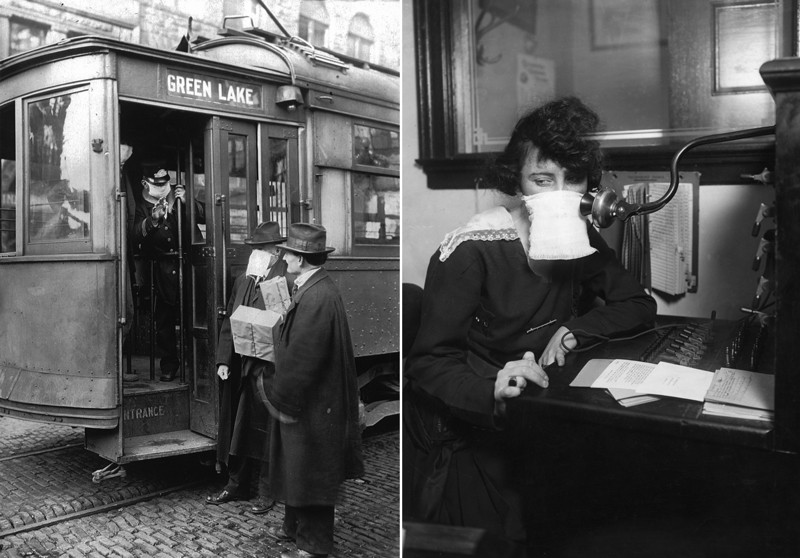
US commuters and telephone operators wore face masks in the 1918 influenza pandemic.Credit: PhotoQuest/Getty; Bettmann/Getty
Jesse Bloom, an evolutionary biologist at the Fred
Hutchinson Cancer Research Center in Seattle, thinks the coronavirus
might follow a similar path. “I do think SARS-CoV-2 will become a less
serious problem and something like flu,” he says. Shaman and others say
the virus could also settle into a seasonal pattern of annual winter
outbreaks similar to flu.
Flu seems to evolve much faster than
SARS-CoV-2, allowing it to sneak past the immune system’s defences. This
feature is why flu vaccines need to be reformulated each year; that
might not be needed for SARS-CoV-2.
Still, the coronavirus might
be able to dodge immunity acquired by infection, and possibly outsmart
vaccines. Already, laboratory studies show that neutralizing antibodies
in the blood of people who have had COVID-19 are less capable of
recognizing a viral variant first identified in South Africa (called
501Y.V2), than variants that circulated earlier in the pandemic4. That is probably because of mutations in the virus’s spike protein, which vaccines target. Trial results suggest that some vaccines might be less effective against 501Y.V2 than against other variants, and some vaccine makers are exploring redesigns of their products.
Still,
the immune system has lots of tricks up its sleeve, and can respond to
many features of the virus, not just spike, says Lavine. “The virus is
probably going to have to go through lots of mutations to make a vaccine
ineffective,” she says. Preliminary trial results also suggest that vaccines can protect people with 501Y.V2 against severe disease, says Rasmussen.
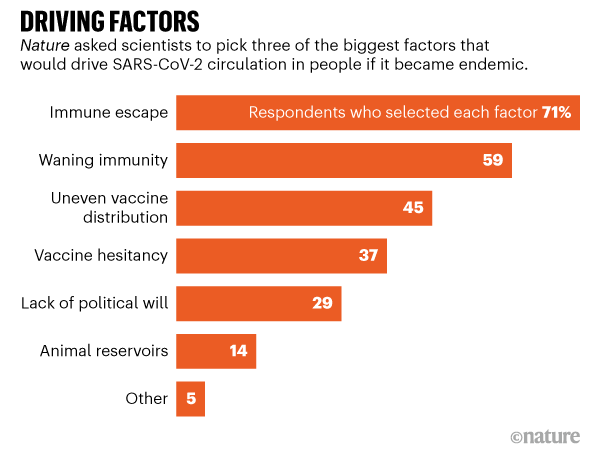
More than 70% of the researchers surveyed by Nature
think that immune escape will be another driver of the virus’s
continuing circulation (see 'Driving factors'). This would not be a
first for a human coronavirus. In a study5
yet to be peer reviewed, Bloom and his colleagues show that the endemic
coronavirus 229E has evolved so that neutralizing antibodies in the
blood of people infected with the viral variant circulating in the late
1980s and early 1990s are much less effective against more recent
variants. People are reinfected with 229E over their lifetime, and Bloom
suspects that it might be harder to stave off the variants that have
evolved to escape previous immunity. But scientists don’t know whether
these reinfections are associated with worse symptoms. “I would expect
that over many years, accumulated mutations to SARS-CoV-2 will more
completely erode neutralizing antibody immunity as we saw for CoV-229E,
although I can’t say for sure how the rates will compare among the two
coronaviruses,” says Bloom.
Source: Nature survey
Bloom thinks it’s probable that SARS-CoV-2 vaccines will
need to be updated, possibly every year. But even then, immunity from
either past vaccination or infection will probably blunt serious
disease, he says. And Lavine notes that even if people are reinfected,
this might not be a big deal. With the endemic coronaviruses, frequent
reinfections seem to boost immunity against related variants and
typically people experience only mild symptoms, she says. But it is
possible that vaccines won’t stop some people developing severe
symptoms, in which case the virus will continue to be a significant
burden on society, says Shaman.
Measles-like virus
If
SARS-CoV-2 vaccines block infection and transmission for life, the
virus might become something akin to measles. “It’s probably less likely
[than other scenarios] but it’s still possible,” says Shaman.
With a highly effective measles vaccine — two doses and a
person is protected for life — the measles virus has been eliminated in
many parts of the world. Before a vaccine was developed in 1963, major
epidemics killed about 2.6 million people, mostly children, a year.
Unlike flu vaccines, the immunization for measles has never needed to be
updated because the virus has yet to evolve in ways that evade the
immune system.
Measles is still endemic in parts of the world with insufficient immunization. In 2018, a global resurgence killed more than 140,000 people.
A similar situation could emerge with SARS-CoV-2 if people decline
vaccines. A survey of more than 1,600 US citizens found that more than
one-quarter would definitely or probably decline a COVID-19 vaccine,
even if it were free and deemed safe (see go.nature.com/3a9b44s).
“How successful we are at addressing those concerns will determine how
many people get the vaccine and how many remain susceptible,” says
Rasmussen.
Animal reservoirs
The future of
SARS-CoV-2 will also depend on whether it establishes itself in a wild
animal population. Several diseases brought under control persist
because animal reservoirs, such as insects, provide chances for
pathogens to spill back into people. These include yellow fever, Ebola
and chikungunya virus.
SARS-CoV-2 probably originated in bats, but
it might have passed to people through an intermediate host. The virus
can readily infect many animals, including cats, rabbits and hamsters.
It is particularly infectious in mink, and mass outbreaks on mink farms
in Denmark and the Netherlands have led to huge animal culls. The virus
has also passed between minks and people. If it became established in a
wild-animal population and could spill back into people, it would be
very difficult to control, says Osterholm. “There is no disease in the
history of humankind that has disappeared from the face of the Earth
when zoonotic disease was such an important part of, or played a role
in, the transmission,” he says.
The path that SARS-CoV-2 might
take to become an endemic virus is challenging to predict, but society
does have some control over it. In the next year or two, countries can
reduce transmission with control measures until enough people have been
vaccinated either to achieve herd immunity or to drastically reduce the
severity of infections. That would significantly reduce deaths and
severe disease, says Osterholm. But if countries abandon strategies to
reduce spread and let the virus reign unchecked then “the darkest days
of the pandemic are still ahead of us”, he says.
Hogan, A. B. et al.Report 33: Modelling the Allocation and Impact of a COVID-19 Vaccine Imperial College London Report https://doi.org/10.25561/82822 (2020).
Will the pandemic go out with a fizzle or a
bang? And what does “living with the virus” actually mean, and when
will we get there?
8 July 2021 – by Linda Geddes
In the UK, it has been dubbed “Freedom Day”. On 19 July, most
remaining COVID-19 restrictions will be lifted, and the world will see
if high rates of COVID-19 vaccination are enough to keep
hospitalisations and deaths from the disease at a stable, and acceptably
low rate.
Some countries, such as New Zealand, have pursued an elimination
strategy, keeping COVID-19 infections close to zero, but at the expense
of heavy travel restrictions and snap lockdowns when outbreaks are
detected. Others, including the UK, have taken the view that SARS-CoV-2
is endemic,
meaning it will continue to circulate in the global population and
trigger outbreaks, but that a certain number of infections and deaths
are tolerable, provided they don’t spiral out of control and overwhelm
the health system, as they have done during peak periods of the
pandemic.
If fully vaccinated individuals do not transmit much virus, and
vaccine coverage is high enough, then even if immunity wanes, regular
booster doses could keep new variants at bay and see the virus
eliminated in some regions of the world.
In other words, for the UK government and others like it, the end of
the COVID-19 pandemic doesn’t mean zero COVID-19, but rather a
transition to a more manageable and predictable level of disease that
can be planned for, such as by allocating a certain number of hospital
beds for COVID-19 patients, and running regular booster vaccination
programmes and public awareness campaigns.
Though they may disagree on the timing, and the level of infections
that might enable a lifting of the restrictions, this is also what many
scientists mean when they talk about “living with the virus”. Once
enough people have been vaccinated, any remaining restrictions on the
freedom of individuals to travel and socialise, or on the ability of
businesses to operate, can be removed, and normal life can resume –
without the threat of health system collapse.
Transition period
Knowing when we’ve reached this point is difficult, however, because
we still don’t know to what extent immunity against the virus wanes over
time, or the degree to which COVID-19 vaccines
prevent transmission. Neither do we know the proportion of the
population each country needs to vaccinate, or to have been infected, to
reach herd immunity – where the whole community becomes protected, and
not just those who are immune.
If fully vaccinated individuals do not transmit much virus, and
vaccine coverage is high enough, then even if immunity wanes, regular
booster doses could keep new variants at bay and see the virus
eliminated in some regions of the world. If they don’t block
transmission, or herd immunity can’t be achieved, the virus will
continue to circulate, but – assuming those who are the most vulnerable
to severe disease have been vaccinated – the number who experience
severe disease may remain acceptably low.
Obtaining definitive answers to these questions will take time, and
given the economic and wider health implications of COVID-19
restrictions, some governments are becoming increasingly impatient.
Removing the brakes
In the UK, where around two thirds
of adults are now fully vaccinated against COVID-19 – including most of
those over the age of 50 and/or with underlying health conditions – the
government plans to lift all remaining restrictions on 19 July.
Although the British Prime Minister Boris Johnson has acknowledged that
this will initially lead to a large increase in coronavirus infections,
his belief is that the UK vaccine rollout has “broken that link between
infection and mortality.” So, although many people may get ill,
hopefully very few will get severely ill or die.
Another uncertainty is the impact of new, more transmissible
SARS-CoV-2 variants, like the Delta variant, which now accounts for most
British infections and is rapidly gaining ground elsewhere. Many UK
scientists would like to see a greater proportion of younger adults, and
possibly many teenagers, fully vaccinated before the remaining
restrictions are removed. This is both to reduce the number of severe
infections in this age group, and because of concerns about “Long
Covid”.
In Israel,
where 56% of the population is now fully vaccinated, most domestic
restrictions were lifted on 1 June, followed by the scrapping of a
requirement to wear facemasks two weeks later. Yet it is now considering
reintroducing some restrictions due to an increase in infections
prompted by the Delta variant. Further variants may yet emerge that
overcome the immunity afforded by vaccination to an even greater extent,
delaying the end to this pandemic even further back. The chances of
this happening are greater the longer a large proportion of the global
population remains unvaccinated, and if infection rates in all countries
remain high.
Acceptable equilibrium
Ultimately though, we will need to learn to live with this virus.
Based on what we know about previous pandemics, COVID-19 should
eventually become less dangerous, and coronavirus infections more
predictable. For instance, the influenza A virus that caused the 1918 Spanish flu pandemic,
which killed more than 50 million people, remained in circulation for
nearly four decades, although it became less virulent for most of this
time. Almost all cases of influenza A since then, have been caused by
descendants of that 1918 virus, but they are no longer as deadly, and
the seasonal flu vaccine further reduces deaths and serious illness from
flu.
Though Boris Johnson is planning a “big bang” reopening on 19 July,
the wider pandemic is unlikely to end with a single big bang, and it is
impossible to set a date for when normality can resume. Rather
infections in different parts of the world may gradually fizzle to the
point where we co-exist with COVID-19 in a perhaps tolerable, if
imperfect, equilibrium.
World
Health Organization experts have warned that even though the
coronavirus pandemic has been very severe, it is “not necessarily the
big one”, and that the world will have to learn to live with Covid-19.
The
“destiny” of the virus is to become endemic, even as vaccines begin to
be rolled out in the US and UK, says Professor David Heymann, the chair
of the WHO’s strategic and technical advisory group for infectious
hazards.
“The world
has hoped for herd immunity, that somehow transmission would be
decreased if enough persons were immune,” he told the WHO’s final media
briefing for 2020.
But
Heymann, who is also an epidemiologist with the London School of
Hygiene and Tropical Medicine, said the concept of herd immunity was
misunderstood.
“It appears the destiny of
SARS-CoV-2 [Covid-19] is to become endemic, as have four other human
coronaviruses, and that it will continue to mutate as it reproduces in
human cells, especially in areas of more intense admission.
“Fortunately,
we have tools to save lives, and these in combination with good public
health will permit us to learn to live with Covid-19.”
The
head of the WHO emergencies program, Dr Mike Ryan, said: “The likely
scenario is the virus will become another endemic virus that will remain
somewhat of a threat, but a very low-level threat in the context of an
effective global vaccination program.
“It
remains to be seen how well the vaccines are taken up, how close we get
to a coverage level that might allow us the opportunity to go for
elimination,” he said. “The existence of a vaccine, even at high
efficacy, is no guarantee of eliminating or eradicating an infectious
disease. That is a very high bar for us to be able to get over.”
That
was why the first goal of the vaccine was to save lives and protect the
vulnerable, Ryan said. “And then we will deal with the moonshot of
potentially being able to eliminate or eradicate this virus.”
Ryan
warned that the next pandemic may be more severe. “This pandemic has
been very severe … it has affected every corner of this planet. But this
is not necessarily the big one,” he said.
“This
is a wake-up call. We are learning, now, how to do things better:
science, logistics, training and governance, how to communicate better.
But the planet is fragile.
“We live in an
increasingly complex global society. These threats will continue. If
there is one thing we need to take from this pandemic, with all of the
tragedy and loss, is we need to get our act together. We need to honour
those we’ve lost by getting better at what we do every day.”
WHO
chief scientist Dr Soumya Swaminathan told the briefing that being
vaccinated against the virus did not mean public health measures such as
social distancing would be able to be stopped in future.
The
first role of the vaccine would be to prevent symptomatic disease,
severe disease and deaths, she said. But whether the vaccines would also
reduce the number of infections or prevent people from passing on the
virus remains to be seen.
“I
don’t believe we have the evidence on any of the vaccines to be
confident that it’s going to prevent people from actually getting the
infection and therefore being able to pass it on,” Swaminathan said. “So
I think we need to assume that people who have been vaccinated also
need to take the same precautions.”
The WHO
director general, Tedros Adhanom Ghebreyesus, said the end of the year
was a time to reflect on the toll the pandemic had taken, but also the
progress made. He said the year ahead would see new setbacks and new
challenges.
“For example, new variants of Covid-19, and helping people who are tired of the pandemic continue to combat it,” he said.
“New
ground has been broken, not least with the extraordinary cooperation
between the private and public sector in this pandemic. And in recent
weeks, safe and effective vaccine rollout has started in a number
countries, which is an incredible scientific achievement.
“This is fantastic, but WHO will not rest until those in need everywhere have access to the new vaccines and are protected.”
(CNN)The coronavirus spreading across the globe could become a constant presence, a leading World Health Organization official has said.
During
a media briefing in Geneva, Dr. Mike Ryan, executive director of the
WHO's health emergencies program, warned Wednesday that the disease may join the mix of viruses that kill people around the world every year.
"This
virus just may become another endemic virus in our communities and this
virus may never go away. HIV hasn't gone away," Ryan said. "I'm not
comparing the two diseases but I think it is important that we're
realistic. I don't think anyone can predict when or if this disease will
disappear."
At a Wednesday briefing, Mike Ryan of the WHO said: "I don't think anyone can predict when or if this disease will disappear."
More than 4.3 million cases of the virus have been recorded worldwide, according to Johns Hopkins University's latest tally.
Multiple teams of scientists around the world are currently trying to develop a viable coronavirus vaccine.
"We
may have a shot at eliminating this virus but that vaccine will have to
be available, it will have to be highly effective, it will have to be
made available to everyone and we'll have to use it," Ryan said. "This
disease may settle into a long-term problem or it may not."
WHO infectious disease epidemiologist Dr. Maria Van Kerkhove struck a more optimistic tone during Wednesday's briefing.
"The
trajectory of this outbreak is in our hands," Van Kerkhove said. "The
global community has come together to work in solidarity. We have seen
countries bring this virus under control. We have seen countries use
public health measures."
WHO Director-General Tedros Adhanom Ghebreyesus echoed that sentiment, adding: "We should all contribute to stop this pandemic."
Forza
Italia sempre più vicina a Italia Viva e alla parte più moderata del Pd.
La Lega è divisa anche al proprio interno. Che fine farà il
centrodestra che abbiamo da sempre conosciuto?
Se Fratelli d’Italia ha scelto una posizione coerente nel dire no al
Governo presieduto da Mario Draghi, Lega e Forza Italia hanno delle
posizioni diverse anche tra loro. Forza Italia è completamente d’accordo
con il premier e sta mostrando un’affinità sempre maggiore con Italia
Viva ed una parte del Partito Democratico. Oramai, Fi è diventata un
partito di centro. Ha perso completamente la sua predisposizione a
guardare a destra e ciò pone fine al suo ruolo di partito federatore del
centrodestra.
Forza Italia potrebbe federarsi con Italia Viva, Azione (il partito
di Carlo Calenda) ed anche il Partito Democratico, o almeno la sua
componente più centrista, e nessuno si sorprenderebbe.
Riguardo a ciò, vi è odore di “Nuova Democrazia Cristiana”.
La Lega, invece, è più sfumata; è in maggioranza ma critica varie
scelte del Governo. Basti pensare alla sua presa di posizione riguardo
all’obbligo vaccinale e al Green Pass. Il leader del Carroccio Matteo
Salvini ha sempre criticato tali scelte, ma cosa pensano i “governisti”
del suo partito, come il ministro Massimo Giorgetti? Salvini potrebbe
avere dei grattacapi anche all’interno del suo stesso partito. Forse,
egli potrebbe avere mantenuto questo atteggiamento sfumato per evitare
il rischio di scissioni.
Solo Fratelli d’Italia ha mantenuto una posizione univoca e coerente
con la sua tradizione. Dal 2012 ad oggi, il partito di Giorgia Meloni è
sempre stato all’opposizione. Esso vuole governare ma vuole governare
con il centrodestra. Questo sta pagando in termini di consenso (che è
aumentato in modo considerevole) e non solo.
Il caso del senatore liberale di Forza Italia Lucio Malan che è
passato a Fratelli d’Italia è paradigmatico. Giorgia Meloni ha
assicurato che il centrodestra sarà compatto. Però, nei fatti,
prevarranno le logiche di coalizione o quelle del Governo? Dunque, ci si
deve porre qualche domanda riguardo al futuro del centrodestra. Fino a
qualche mese fa, il centrodestra sembrava essere imbattibile. Oggi,
invece, la partita è aperta ed i sondaggi sulle elezioni amministrative
sembrano confermare ciò. Siamo di fronte ad un harakiri del
centrodestra?
















{kind=link}